Vermont, long regarded for its bucolic landscapes and small-town charm, is experiencing a health care bottleneck that is intensifying across the state: rising emergency room wait times. What was once a dependable system of quick, if modest, urgent care has become a frustrating exercise in patience for many residents, even in rural areas where health care delivery was traditionally viewed as community-oriented and accessible.
The story unfolding across Vermont’s emergency departments (EDs) reflects a broader national trend, but the Green Mountain State presents unique variables that complicate both the causes and the solutions. The uptick in wait times is not driven by a single issue but rather by a convergence of systemic healthcare challenges, labor shortages, shifting demographics, and a post-pandemic recalibration of care-seeking behavior.
Vermont Hospitals with Shortest Wait Times
Below are five hospitals in Vermont with the shortest emergency room wait times:
- 🥇 Grace Cottage Hospital has the shortest average ER wait time at 2.1 hours in Vermont
- 🥈 Northwestern Medical Center, with an average wait time of 2.6 hours, ranks second for the shortest ER wait time in Vermont
- 🥉 Central Vermont Medical Center, with an average wait time of 2.7 hours, ranks third for the shortest ER wait time in Vermont
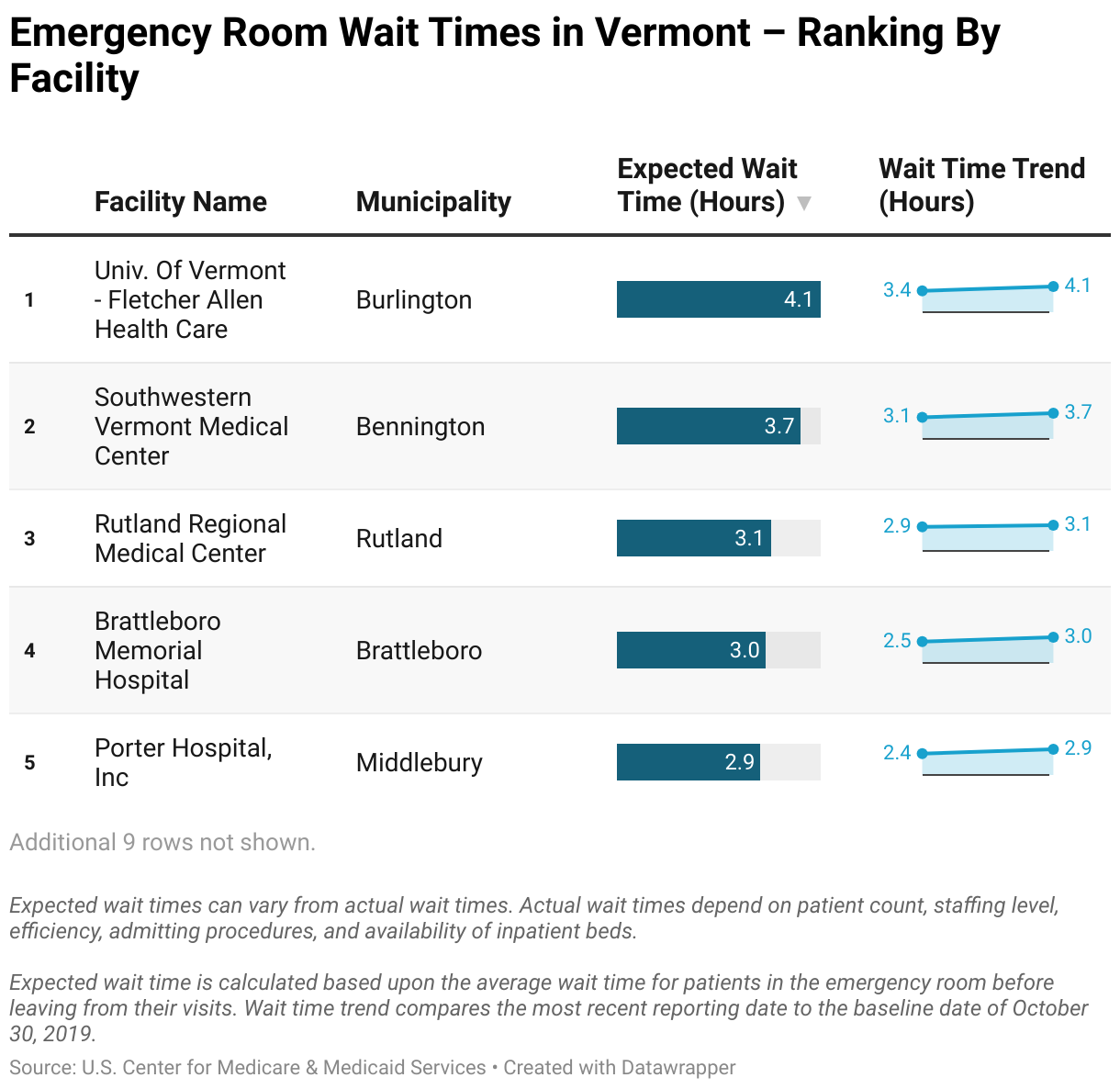
Vermont Hospitals with Longest Wait Times
Below are five hospitals in Vermont with the longest emergency room wait times:
- 🐌 University of Vermont Medical Center has the longest average ER wait time at 4.1 hours in Vermont
- 🐢 Southwestern Vermont Medical Center, with an average wait time of 3.7 hours, ranks second for the longest ER wait time in Vermont
- 🦥 Rutland Regional Medical Center, with an average wait time of 3.1 hours, ranks third for the longest ER wait time in Vermont
Workforce Shortages Amplify the Problem
Vermont’s health care workforce has been in a state of attrition for years, but the COVID-19 pandemic accelerated the exodus of nurses, technicians, and physicians from the industry. Rural hospitals, already operating with lean staff, have struggled the most. Positions that once attracted Vermont-trained nurses and clinicians are now increasingly filled by expensive travel nurses and temporary contract workers, leading to higher costs without necessarily improving care continuity.
This workforce instability affects the emergency department uniquely. EDs require 24/7 staffing and must be prepared for a wide range of medical scenarios, from pediatric fever spikes to cardiac arrests. A thin staff not only slows the triage and treatment process but also contributes to burnout, leading to a cyclical pattern of departures and understaffing.
In response, some hospitals have attempted to consolidate services or redirect patients to urgent care clinics, but these facilities often lack the diagnostic tools or specialists needed for more serious conditions. The result is a funneling effect back into the emergency departments, even for non-emergency care.
The Behavioral Health Bottleneck
An increasingly visible driver of emergency room crowding in Vermont is the rise in behavioral health emergencies. With limited access to psychiatric services statewide and a dearth of inpatient psychiatric beds, individuals experiencing mental health crises often have no choice but to seek help at the emergency room.
Many of these patients end up staying for extended periods—some for several days—while awaiting placement in a psychiatric facility. Vermont’s designated mental health agencies and the state-run Vermont Psychiatric Care Hospital are both operating under significant strain, and community support systems often lack the bandwidth to prevent escalation before a crisis occurs.
The Vermont Department of Mental Health has acknowledged this systemic problem and is working to expand crisis response programs and mobile mental health units, but these initiatives are in early stages and have yet to yield significant reductions in ED boarding times for psychiatric patients.
Post-Pandemic Patient Behavior
Compounding the problem is a shift in how Vermonters use emergency services. During the height of the pandemic, many delayed care for chronic conditions or postponed elective procedures. As those patients reenter the health care system, many arrive at emergency rooms in more advanced stages of illness, requiring more complex and time-consuming care.
Moreover, some residents, particularly those in rural and underserved regions, have grown increasingly reliant on emergency departments as a de facto primary care solution. Vermont has a shortage of primary care physicians, and wait times for routine appointments can stretch weeks, pushing patients with pressing but non-life-threatening conditions to seek immediate attention in emergency departments.
Telehealth was once seen as a promising solution, especially during the pandemic, but its usage has declined amid regulatory uncertainties and a lack of broadband access in parts of rural Vermont. As a result, many residents revert to the most accessible—and often only—immediate care option: the emergency room.
Infrastructure and Technology Constraints
Unlike some larger states that have invested heavily in emergency department redesign and predictive analytics, Vermont’s hospitals—many of which were built decades ago—struggle to modernize their physical spaces. Limited infrastructure hampers their ability to create dedicated fast-track lanes for less critical patients or to implement sophisticated tracking systems that optimize staff deployment and patient flow.
Electronic health record (EHR) systems, while broadly adopted, remain a source of inefficiency for some providers. Disparate systems between hospitals, clinics, and long-term care facilities create documentation lags and communication breakdowns that further slow down the discharge or transfer process.
In some hospitals, small pilot programs have been introduced to streamline intake procedures, use remote triage for certain patients, and employ data analysis to predict peak times. But these initiatives are typically small in scope, and the financial limitations of nonprofit hospital systems restrict their scalability.
Legislative and Policy Approaches
State policymakers have attempted to address the issue through both funding and regulatory reform. The Green Mountain Care Board, Vermont’s health care regulatory authority, has launched studies and listening sessions to understand ED bottlenecks and explore innovative models of care. One effort involves enhancing integration between hospitals and community-based health providers, particularly in behavioral health.
In 2023, the Vermont legislature passed measures to increase Medicaid reimbursement rates for mental health services and expand the availability of nurse practitioners and physician assistants in underserved areas. These efforts are intended to improve upstream care access and reduce reliance on emergency services. However, the full impact of these changes may take several years to materialize.
There is also discussion around building new facilities or expanding existing ones, particularly for mental health care, but community opposition, environmental permitting, and budget constraints have slowed progress.
Rural-Specific Challenges
Vermont’s rural geography complicates nearly every aspect of emergency care delivery. Ambulance coverage is sparse in some areas, and transport times to hospitals can stretch beyond an hour. Small hospitals, often the only medical facility within dozens of miles, face the dual burden of serving as both emergency and primary care centers.
In places like Newport or Middlebury, even a modest increase in patient volume can overwhelm capacity. And when patients need to be transferred to a higher-level facility, such as Dartmouth-Hitchcock in New Hampshire or UVM Medical Center, bed availability and transport coordination create further delays.
Rural hospital closures—an issue looming in many parts of the U.S.—have not yet materialized in Vermont, but financial instability is a pressing concern. Many facilities are operating on razor-thin margins, making it difficult to invest in staff or modernization.
The Human Cost
While metrics and policy debates frame much of the conversation around emergency room wait times, the human consequences are deeply felt. Long waits can exacerbate medical conditions, heighten anxiety, and erode trust in the health care system. For some patients—especially elderly individuals, people with disabilities, or those with limited English proficiency—long emergency room stays can be both physically exhausting and emotionally isolating.
There is also the hidden cost to providers. Emergency department staff in Vermont frequently describe high stress levels, emotional fatigue, and moral distress from not being able to deliver timely care. Nurse retention remains an ongoing concern, and recruitment efforts must compete not only with other hospitals but with industries that offer less demanding schedules and better compensation.
Better Emergency Care for Vermont
Improving emergency room wait times in Vermont will require a multipronged strategy: expanding access to primary and behavioral health care, investing in workforce development, and modernizing hospital infrastructure. It will also require a cultural shift in how emergency departments are used—and a renewed effort to educate patients about alternative options for care.
There is no quick fix to Vermont’s ED backlog, but incremental progress is possible. The state’s strong track record of health care reform, its compact size, and its engaged medical community offer a foundation for meaningful change. The question is not whether Vermont can address the problem, but whether it can do so before the situation becomes a more entrenched crisis.
For now, patients across the state will continue to wait—some patiently, others in pain—for a system that can catch up with their needs.