In recent years, the issue of prolonged emergency room (ER) wait times has emerged as a critical challenge across the United States. Rhode Island, the smallest state by area, has not been immune. Despite its compact geography and relatively dense healthcare infrastructure, Rhode Island’s emergency departments have experienced sustained pressures that are stretching patient wait times and exposing deeper systemic inefficiencies in the state’s healthcare delivery network.
Rhode Island’s healthcare system, anchored by several key institutions including Lifespan, Care New England, and independent hospitals, has historically been a source of pride for residents and policy leaders alike. However, the aftershocks of the COVID-19 pandemic, coupled with staffing shortages and rising patient volumes, have eroded the responsiveness of its emergency care. Today, Rhode Island ranks among the states with some of the longest average ER wait times, a development that has both patients and healthcare administrators sounding alarms.
Rhode Island Hospitals with Shortest Wait Times
Below are five top hospitals in Rhode Island which have the shortest emergency room wait times:
- 🥇 Westerly Hospital has the shortest average ER wait time at 1.9 hours in Rhode Island
- 🥈 Our Lady Of Fatima Hospital, with an average wait time of 3.1 hours, ranks second for the shortest ER wait time in Rhode Island
- 🥉 Women & Infants Hospital of Rhode Island, with an average wait time of 3.3 hours, ranks third for the shortest ER wait time in Rhode Island
- Newport Hospital, with an average wait time of 3.4 hours, ranks fourth for the shortest ER wait time in Rhode Island
- Roger Williams Medical Center, with an average wait time of 3.6 hours, ranks fifth for the shortest ER wait time in Rhode Island
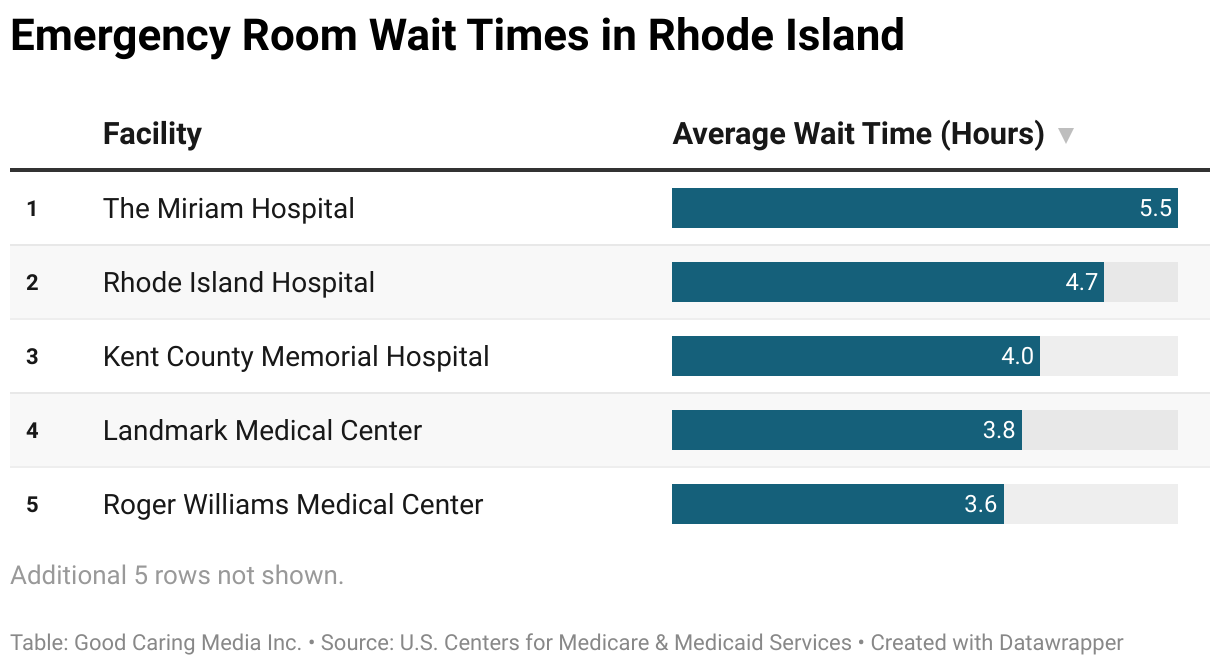
Rhode Island Hospitals with Longest Wait Times
Below are five top hospitals in Rhode Island which have the longest emergency room wait times:
- 🐌 The Miriam Hospital has the longest average ER wait time at 5.5 hours in Rhode Island
- 🐢 Rhode Island Hospital, with an average wait time of 4.7 hours, ranks second for the longest ER wait time in Rhode Island
- 🦥 Kent County Memorial Hospital, with an average wait time of 4.0 hours, ranks third for the longest ER wait time in Rhode Island
- Landmark Medical Center, with an average wait time of 3.8 hours, ranks fourth for the longest ER wait time in Rhode Island
- Roger Williams Medical Center, with an average wait time of 3.6 hours, ranks fifth for the longest ER wait time in Rhode Island
A Statewide Struggle
According to recent data from the Centers for Medicare & Medicaid Services (CMS) and hospital-level reporting, Rhode Island emergency departments are seeing average wait times before admission—referred to as “door-to-admit” times—that often exceed national benchmarks. Patients in Rhode Island frequently wait several hours before even being seen by a physician, and those requiring hospital admission can experience much longer delays before receiving inpatient care.
At some of the state’s busiest hospitals, such as Rhode Island Hospital in Providence and Kent Hospital in Warwick, median wait times have at times topped six to eight hours. In some isolated cases during peak surges, those numbers have reached upwards of 12 hours. While these extended periods reflect the broader national struggle with healthcare access, they also highlight unique local constraints.
Staffing and Capacity Challenges
One of the central drivers behind the rising ER wait times is a persistent staffing shortage. Registered nurses, emergency physicians, technicians, and support staff have all become increasingly difficult to recruit and retain. Burnout, particularly in the wake of the pandemic, has pushed many healthcare workers out of the profession entirely or into less demanding roles. Rhode Island, with its high cost of living and relatively modest healthcare wages compared to neighboring Massachusetts, faces an uphill battle in this workforce competition.
In addition to staffing limitations, capacity constraints are also impeding ER efficiency. Rhode Island hospitals frequently operate near or at full capacity, particularly in urban centers. When inpatient beds are unavailable, emergency rooms become de facto holding units for admitted patients, preventing new arrivals from being seen promptly. This phenomenon, known as “boarding,” creates a cascading bottleneck: admitted patients remain in the ER, occupying beds and drawing on staff resources, which in turn prevents new patients from receiving timely care.
Moreover, mental health crises have contributed significantly to capacity burdens. Patients in psychiatric distress often require specialized placements, and such beds are in critically short supply across Rhode Island. As a result, behavioral health patients can remain in ERs for days, awaiting transfer to appropriate care settings—further exacerbating delays for all patients.
Role of Primary and Urgent Care Access
ERs have long served as a safety net for individuals without regular access to primary or urgent care. In Rhode Island, disparities in access to outpatient services have contributed to inappropriate or avoidable ER visits. Communities with limited healthcare options—often in economically disadvantaged areas—are more likely to use emergency services for non-emergency needs.
Though Rhode Island boasts a relatively high rate of insured residents due to Medicaid expansion and state-level policy initiatives, insurance coverage does not necessarily guarantee access to a provider. Patients often face long waits for primary care appointments or lack transportation to reach those providers, resulting in default reliance on the ER for medical needs that could otherwise be managed in outpatient settings.
This dynamic places additional strain on emergency departments, where staff are obligated to triage and treat every incoming patient, regardless of the severity of the condition. Consequently, patients with more urgent or life-threatening issues face extended delays as providers work through a broader spectrum of health needs.
Financial and Administrative Pressures
Hospitals in Rhode Island are also navigating complex financial challenges. Reimbursement rates, particularly for Medicaid patients, often do not cover the full cost of emergency care. This has led some systems to operate with thin margins, limiting their ability to invest in expanded facilities or staffing. Administrative burdens, such as prior authorizations and documentation requirements, further slow down throughput and discharge processes, compounding delays.
Hospital consolidation, while intended to streamline operations and improve care coordination, has produced mixed outcomes. The merging of systems such as Lifespan and Care New England, although not fully realized, reflects ongoing efforts to address fragmentation. Yet, during periods of transition, operational uncertainties can lead to inconsistencies in staffing, IT infrastructure, and patient handoff procedures—all of which contribute to ER inefficiencies.
Policy Interventions and Legislative Oversight
State policymakers have taken notice of the growing crisis in emergency care. The Rhode Island Department of Health has initiated efforts to improve data transparency and coordinate regional emergency response strategies. Additionally, the General Assembly has considered measures aimed at expanding behavioral health infrastructure, increasing Medicaid reimbursement rates, and bolstering the healthcare workforce pipeline through incentives and loan forgiveness programs.
One such initiative involves partnerships with local colleges and universities to accelerate the training of nurses and allied health professionals. Another focuses on the development of mobile crisis units, designed to divert mental health patients away from ERs and toward more appropriate care environments. These efforts, while promising, remain in early stages and will require sustained funding and oversight.
At the federal level, Rhode Island has also benefited from grant funding tied to the American Rescue Plan and other COVID-19 relief packages, some of which have been earmarked for improving emergency care delivery. The state’s congressional delegation continues to advocate for further investment in healthcare infrastructure, arguing that systemic weaknesses revealed during the pandemic must be addressed through long-term strategic planning.
The Human Cost of Delay
While statistics and policy frameworks shape the contours of the ER wait time discussion, the human dimension is inescapable. Patients experiencing severe pain, trauma, or psychological distress often endure hours of uncertainty before receiving attention. Families are left anxious, confused, and frustrated by opaque triage processes and extended delays.
These experiences erode public trust in healthcare institutions. For vulnerable populations—such as the elderly, the uninsured, or those with chronic conditions—long ER waits can lead to worsened outcomes, hospital readmissions, or avoidable complications. For healthcare workers, the emotional toll of operating in high-stress, resource-constrained environments contributes to burnout and turnover, further entrenching the cycle.
Better Emergency Care for Rhode Island
Rhode Island stands at a crossroads in confronting its emergency room wait time crisis. While small in size, the state faces a confluence of challenges that mirror national trends, magnified by localized resource limitations and workforce vulnerabilities. Addressing these issues will require a coordinated approach that transcends individual hospital systems and engages public health, primary care, behavioral health, and policy communities.
The solutions are unlikely to be swift or singular. Rather, incremental progress across multiple fronts—workforce development, infrastructure expansion, digital innovation, and equity in access—will be essential in restoring balance to Rhode Island’s emergency care system.
For now, ER wait times remain a barometer of systemic stress, a visible symptom of deeper strains within the healthcare continuum. How Rhode Island chooses to respond in the coming years may well determine not only the health of its hospitals, but also the broader well-being of the communities they serve.