In the intricate and high-stakes landscape of American health care, few arenas reflect the system’s challenges as clearly as the emergency room. In Maryland, a state with a mix of dense urban centers and sprawling rural communities, the issue of emergency room (ER) wait times has become a pressing concern for patients, providers, and policymakers alike. The state has earned the unwelcome distinction of having some of the longest ER wait times in the nation, a trend that has proven resistant to reform despite repeated efforts to improve performance and patient outcomes.
This article explores the complex web of factors contributing to prolonged ER wait times in Maryland, the systemic pressures that sustain them, and the solutions that are either underway or under consideration. As the state navigates a post-pandemic world, its ERs serve as both frontline care facilities and barometers of a system nearing capacity.
Maryland Hospitals with Shortest Wait Times
Below are five hospitals in Maryland with the shortest emergency room wait times:
- 🥇 Atlantic General Hospital has the shortest average ER wait time at 2.5 hours in Maryland
- 🥈 University Of Maryland Shore Medical Center At Chestertown, with an average wait time of 2.7 hours, ranks second for the shortest ER wait time in Maryland
- 🥉 Garrett Regional Medical Center, with an average wait time of 2.8 hours, ranks third for the shortest ER wait time in Maryland
- University Of Maryland Harford Memorial Hospital, with an average wait time of 3.0 hours, ranks fourth for the shortest ER wait time in Maryland
- Walter Reed National Military Med Center, with an average wait time of 3.0 hours, ranks fifth for the shortest ER wait time in Maryland
Maryland Hospitals with Longest Wait Times
Below are five hospitals in Maryland with the longest emergency room wait times:
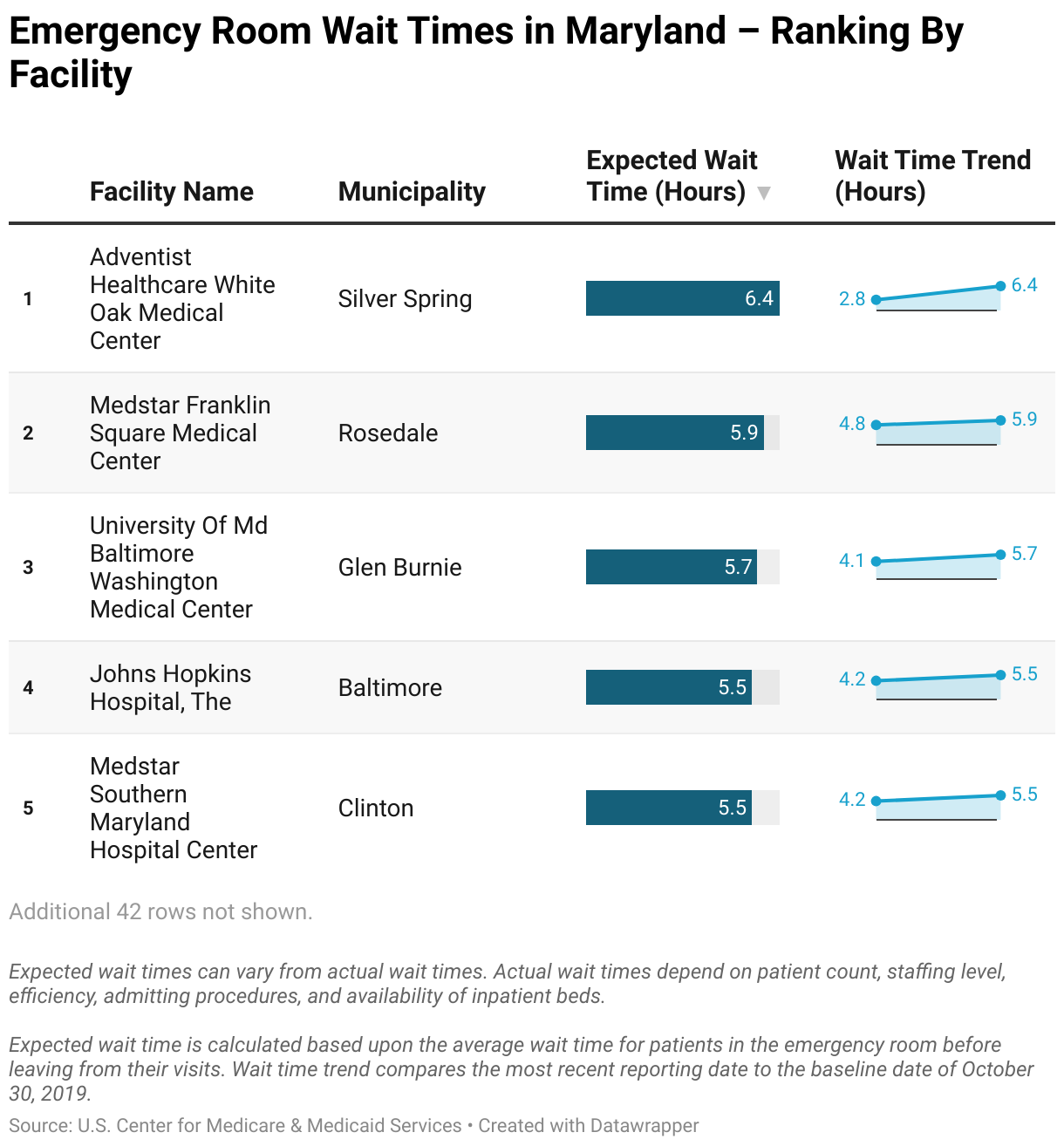
- 🐌 Adventist Healthcare White Oak Medical Center has the longest average ER wait time at 6.4 hours in Maryland
- 🐢 MedStar Franklin Square Medical Center, with an average wait time of 5.9 hours, ranks second for the longest ER wait time in Maryland
- 🦥 University Of Maryland Baltimore Washington Medical Center, with an average wait time of 5.7 hours, ranks third for the longest ER wait time in Maryland
- The Johns Hopkins Hospital, with an average wait time of 5.5 hours, ranks fourth for the longest ER wait time in Maryland
- MedStar Southern Maryland Hospital Center, with an average wait time of 5.5 hours, ranks fifth for the longest ER wait time in Maryland
Root Causes of the Crisis
The underlying causes of Maryland’s prolonged ER wait times are multifaceted. Foremost among them is the state’s unique hospital funding structure. Maryland operates under a Global Budget Revenue (GBR) system, a model developed in partnership with the federal government that caps annual hospital revenues in an effort to control costs and incentivize preventative care. While the system has succeeded in limiting unnecessary admissions and reducing duplicative testing, it has also created unintended consequences in emergency care.
Under the GBR model, hospitals have less financial incentive to quickly admit ER patients, since doing so does not increase revenue. As a result, patients may remain in ER beds for longer periods while awaiting transfer to inpatient units, even when such transfers are medically indicated. This phenomenon, known as “boarding,” effectively blocks ER beds from serving new arrivals and contributes to the growing queue of waiting patients.
The boarding problem is exacerbated by statewide staffing shortages. Like much of the country, Maryland has seen a decline in the number of available nurses and other clinical support staff, a trend intensified by the COVID-19 pandemic and its aftermath. Burnout, early retirement, and a competitive national job market have all thinned the workforce, limiting the capacity of hospitals to move patients efficiently through the system.
Compounding the issue is the closure of several community hospitals and the consolidation of health systems in recent years. As facilities shutter or merge, the remaining hospitals must serve a larger geographic area and absorb greater patient volume, straining resources and lengthening response times. In rural parts of the state, access to emergency care has become particularly tenuous, often requiring long travel distances even before a patient enters the ER queue.
Urban Centers Under Pressure
Nowhere are the effects of prolonged ER wait times more acute than in Maryland’s urban centers, particularly Baltimore City. The city’s hospitals, including some of the state’s most prominent academic medical centers, routinely report ER overcrowding and long delays for both urgent and non-urgent cases.
The demographic profile of these urban areas—characterized by higher rates of chronic illness, poverty, and violence—means that ERs frequently serve as primary care providers by default. Patients who lack regular access to healthcare often turn to emergency rooms for issues that might otherwise be managed through outpatient services. The result is a steady influx of non-emergency cases that compound delays and frustrate triage efforts.
Hospitals in these areas also contend with frequent ambulance diversions, a practice in which hospitals temporarily refuse to accept new ambulance arrivals due to capacity issues. This practice has ripple effects across the system, leading to longer transport times and extended on-site waiting periods as emergency medical services (EMS) personnel remain with patients until care can be transferred.
Patient Experience and Health Outcomes
For patients, the consequences of long ER wait times are far more than an inconvenience. Prolonged waits can lead to poorer health outcomes, particularly for those with time-sensitive conditions such as strokes, heart attacks, or severe infections. Delays in treatment increase the risk of complications, lengthen hospital stays, and can contribute to preventable mortality.
Even for less urgent cases, extended waiting can cause pain, anxiety, and dissatisfaction. Surveys consistently show that long ER waits are among the top complaints cited by hospital patients. These negative experiences not only affect patient morale but also influence a hospital’s reputation, potentially deterring individuals from seeking care when needed.
For the uninsured and underinsured, who are already vulnerable, the ER may represent the only point of contact with the healthcare system. When that entry point is delayed or inefficient, it deepens existing disparities and erodes trust in the system’s ability to deliver equitable care.
Policy Responses and Innovations
Efforts to address Maryland’s ER wait time crisis have been varied. At the state level, health officials have introduced regulatory adjustments to the GBR system in an attempt to better account for ER flow dynamics. These include measures to encourage faster inpatient admissions from the ER and to penalize excessive boarding.
Hospitals themselves have invested in triage modernization, including fast-track lanes for lower-acuity patients, expanded use of nurse practitioners and physician assistants, and digital check-in tools designed to expedite the registration process. Telemedicine has also emerged as a potential relief valve, enabling some patients to receive virtual consultations that may obviate the need for an ER visit altogether.
In Baltimore, pilot programs have aimed to redirect non-emergency cases away from ERs through expanded urgent care centers and community health initiatives. Some of these programs have shown promise in reducing overall ER volume, but scaling them statewide remains a logistical and financial challenge.
Meanwhile, federal funding through the American Rescue Plan and other pandemic-era relief efforts has allowed some hospitals to temporarily bolster staff levels and expand capacity. However, these interventions are often short-term and unsustainable without longer-term structural change.
Better Emergency Care for Maryland
As Maryland continues to grapple with its ER wait time crisis, the broader implications for healthcare delivery cannot be ignored. Long wait times are symptomatic of deeper systemic issues—resource allocation, care accessibility, and workforce sustainability among them. Addressing these challenges will require a coordinated effort across multiple stakeholders, from hospital administrators and frontline providers to state regulators and federal agencies.
The state’s ambitious experiment with hospital budgeting has yielded both accolades and criticisms. While it remains a model for cost containment, its impact on emergency care demands further scrutiny and adjustment. Ensuring that cost savings do not come at the expense of timely access to life-saving treatment is a delicate but necessary balancing act.
In the end, the emergency room remains a linchpin of the healthcare system—a place where critical decisions are made and lives are saved under immense pressure. For Maryland, ensuring that this vital institution operates effectively is not only a matter of logistics but of public trust and moral obligation. The state’s success in tackling its ER wait time problem will serve as a benchmark for other states navigating similar challenges and will shape the future trajectory of emergency care nationwide.